

Scoliosis is a term that describes changes in the shape and position of the spine, thorax, and trunk. When viewed from behind, the spine may curve side to side and rotate, making it appear more like an “S” or “C” shape instead of being straight.
Causes of Scoliosis
About 20% of scoliosis cases are due to underlying conditions or other causes. These include:
- Congenital: Vertebrae are not properly formed.
- Neuromuscular: Conditions like Spinal Muscle Atrophy.
- Syndromic: Associated with syndromes such as Marfan Syndrome or Ehlers-Danlos Syndrome.
- Other Causes: Such as post-surgical complications.
The remaining 80% of cases are idiopathic, meaning the exact cause is unknown. Idiopathic scoliosis is typically classified by using a combination of the Cobb angle (more on this later), age, and location of the curve.
This blog focuses on idiopathic scoliosis in adolescents and adults, as it represents the majority of cases.
Fact 1: Posture Alone Cannot Diagnose Scoliosis
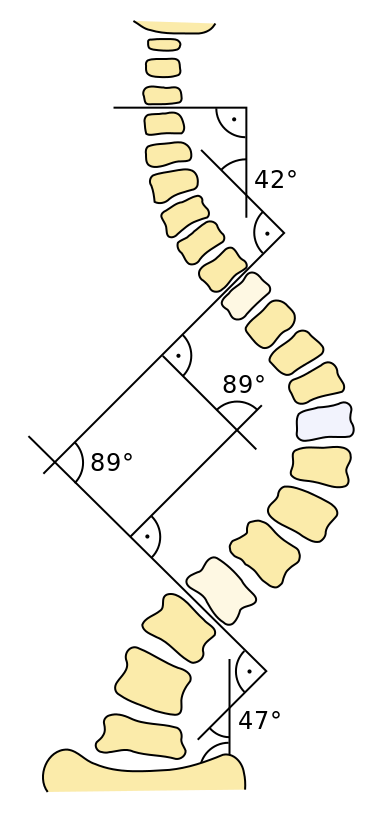
While observing someone’s standing or moving posture (commonly called the Adam’s test) might suggest scoliosis, it is not sufficient for a diagnosis. Diagnosis requires an X-ray to measure the Cobb angle, which is the angle formed between the two most tilted vertebrae. Scoliosis is confirmed if this angle is 10° or higher and axial rotation of the spine is present (Negrini et al. 2018).
Fact 2: Scoliosis Progression in Adults
For adults, low to moderate scoliosis rarely progresses:
- Curves less than 10° are not considered scoliosis.
- Curves under 30° typically remain stable throughout adulthood.
- Curves above 30° have an increased risk of progression.
- Curves greater than 50° almost certainly progress (Negrini et al. 2018).
For adolescents, treatment is guided by the Cobb angle and growth potential. Curves under 25° usually require observation, while curves between 25° and 45° might need bracing. More severe cases may require surgery, depending on various factors such as curve severity and remaining growth.
Fact 3: No “Best” Exercise for Scoliosis
A variety of exercises are suggested for scoliosis, including breathing drills, spine stretches, and back strengthening. While these exercises can improve strength, function, and symptom relief, research shows they are not effective in reducing the Cobb angle or preventing curve progression in adolescent scoliosis.
Studies like Day et al. 2019 and Fan et al. 2020 suggest insufficient evidence that scoliosis-specific exercises effectively improve Cobb angles. However, general exercise is still beneficial for overall function and perceived status (Scheiber et al. 2019). The type of exercise does not significantly impact outcomes, making it important to choose activities you enjoy to ensure long-term adherence.
Fact 4: Scoliosis Does Not Cause Back Pain
According to the Scoliosis Research Society, adolescents with scoliosis experience back pain at the same rate as their peers without scoliosis. Adults with curves less than 30° also have similar back pain risks as those without scoliosis.
Back pain is influenced by numerous factors, including behavior, lifestyle, social, and psychological aspects (Cholewicki et al. 2019). Addressing factors within your control, such as physical activity, stress reduction, and sleep improvement, can significantly impact pain and function.
Fact 5: All Activities Are Permissible

The International Society of Scoliosis Orthopaedic and Rehabilitation Treatment recommends that individuals with scoliosis remain active in sports and other activities, as participation does not affect scoliosis occurrence or severity.
Notable athletes with scoliosis include Lamar Gant, a world record-holding powerlifter; Jessica Ashwood, an Olympic swimmer; and Usain Bolt, an Olympic sprinter. These examples illustrate that scoliosis does not limit high-level athletic performance.
Summary
Key takeaways about scoliosis:
- Diagnosis: Cannot be confirmed by posture alone; requires X-ray measurement of the Cobb angle.
- Progression: Rarely progresses in adults with low to moderate scoliosis.
- Exercise: No single best exercise; general exercise is beneficial for overall function.
- Pain: Scoliosis of low to moderate severity does not cause back pain; multiple factors contribute to pain.
- Activity: No exercise or activity is off-limits; remaining active is highly encouraged.
Disclaimer
Experiences may vary, and that’s okay. This blog aims to provide the latest research, emphasizing that individuals with scoliosis can still lead active, healthy lives.


